


Greenstick fractures
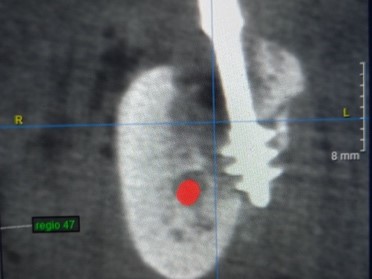
Fig. 1 Unnoticed chipping of a bone fragment during the insertion of a Corticobasal® implant in IF Method 5a. The implant shown here is 100% stable, there were no clinical abnormalities at any time.
Internationale Implantatstiftung
Wir sind eine gemeinnützige und wissenschaftlich ausgerichtete Stiftung des Privatrechts, die Patientenerfahrungen und Ergebnisse von
Zahnimplantat-Versorgungen nach Knochenaufbau
erfassen und bewerten möchte.
Ziel ist die Erstellung einer Studie zur dentalen Versorgungsrealität in Deutschland / Österreich / Schweiz.
Einsender (Patienten u.a.) erhalten eine fachliche Einschätzung und Bewertung, kostenfrei und vertraulich.
Bitte wenden Sie sich an:
Internationale Implantatstiftung München
contact@implantfoundation.org
Creation of this 002-Version: IF Board
Applicable documents: All IF Consensus Documents No. 1 – 7;
AO Principles of Fracture Management; THOMAS P RÜEDI, RICHARD BUCKLEY, CHRISTOPHER G MORAN; ISBN 9781588905567
Scope: Lateral and screwable oral and craniofacial implants according to IF Consensus Document No. 1
A „corrective intervention“ serves to correct undesired developments or conditions in a BIPS. A distinction is made between surgical and prosthetic corrective interventions. Sometimes corrective interventions are supported by drug therapy to reduce the chewing force.
The need for corrective surgery does not imply that the basic treatment was defective or wrong.
The incomplete or omitted implementation of a necessary corrective intervention is a treatment mistake.
Whenever corrective prosthetic interventions are performed, the stability of all implants involved must be checked and authorized specialists must be available to carry out the surgical part of the necessary corrective intervention.
Resting phase: The period of time during which the prosthetic construction should not be removed due to the known bone remodeling and the associated bone weakness. This period is between 12 and 24 months after the first intervention. Earlier corrective interventions should be carried out only by the treatment provider who has performed the initial treatment.
BIPS: Bone-Implant-Prosthetic-System
(see IF Consensus Document No. 7, www.implantfoundation.org)
Surgical corrective interventions are carried out
Combined surgical and prosthetic corrective interventions are performed when an “overload osteolysis” is diagnosed. This osteolysis can be initially sterile. However, it can later be accompanied by an infection if it remains untreated for a longer period of time.
While peri-implantitis (PI; as associated with conventional, 2-phase dental implants) would affect the crestal parts of the implant, an overload osteolysis affects the load-bearing parts (threads or baseplates), predominantly when the threads are not, or only partially, anchored in the 2nd/3rd cortical. Such an overload osteolysis usually occurs within two years after implant placement and can progress/propagate over the arch to general instability of the construct of all or almost all implants (propagating overload). Initially a prosthetic corrective intervention can be assumed to be sufficient to solve the problem. If this intervention is not performed, the problem will exacerbate.
For technical reasons, the occasional splintering off of parts of the cortical is unavoidable and usually goes unnoticed. The apical parts of the threads of Corticobasal® implants are larger than the drilling that is carried out before the implants are inserted. This problem is not limited to Corticobasal® implants, but affects all implants that are inserted into the bone with the aim of achieving great primary stability, i.e. all compression screws.
An orthograde infection of the bone after Greenstick fractures along the axis of Corticobasal® implants is possible and usually leads to sequestration. If these sequestra do not work their way through the mucous membrane of their own accord, they should be removed. A wait-and-see attitude is generally indicated.
Greenstick fractures
Fig. 1 Unnoticed chipping of a bone fragment during the insertion of a Corticobasal® implant in IF Method 5a. The implant shown here is 100% stable, there were no clinical abnormalities at any time.
Procedure: In the context of surgical corrective interventions, single, several or even all implants are replaced and in selected cases an immediate replacement of these implants may be tried (aim of treatment) by very experienced, authorized treatment providers.
Indications:
It may be necessary to make changes to the prosthetic construction during the “resting phase” (i.e. the period when no removal of the prosthetic construction is to be made). Reasons for such prosthetic changes include the following circumstances:
It is not indicated to remove the bridge within the first 12-24 months after the basic treatment. In the case of prosthetic problems that cannot be solved by grinding or building up the occlusal surfaces, cemented over-bridges must be inserted. The first bridge must not be removed during the initial healing phase.
Simple separating bridges on Corticobasal® implants is a malpractice.
A simple corrective procedure is carried out if one or more implants are removed while leaving the prosthetic construction intact. To do this, one or more implants are separated horizontally from the prosthetic construction with a carbide cutter and they are then unscrewed. The indication for such implant removal results from a blackening of the bone around the force-transmitting thread areas as described in IF Consensus Document No. 1.
Provided the construction is stable, individual implants can be removed without replacing them, as they have not been actively involved in the load-transmission of the BIPS for a long time. In this situation, the other implants have successively (and often for a long time) taken over the load transmission tasks of the no longer integrated implant. In any case, implants in strategic positions should be replaced.
Corrective procedures are complex when the prosthetic construction and numerous implants in a jaw need to be removed and replaced.
The aim of this corrective intervention is the complete re-creation of an implant base for a BIPS with subsequent restoration with immediate loading.
Multi-stage corrective interventions are to be planned if a sufficient number of stable implants could be inserted during the first corrective intervention, but it is to be expected that not all implants will retain stable bone-implant contact.
Reasons to believe that there is a loss of bone-implant contact can be:
If there are reasons that lead to the assumption that one or more implants will have to be replaced again after a short healing phase, a milled plastic bridge is used as an interim restoration with a firm, definitive cement after the first corrective intervention. The usage of temporary cements is in general contra-indicated in all cases of such corrective interventions. Further treatment takes place after approx. 3 months.
As part of the 2nd corrective surgery, mobile implants are removed and replaced, and the total number of implants should be increased as much as possible. This approach is possible because the jawbone has been able to recover and consolidate in the meantime.
With this approach, the aim of the first corrective intervention is to achieve at least threepoint-support that allows the insertion of a fixed bridge so that, during the bone‘s healing phase (i.e. until a sufficient number of implants can be placed in immediate loading protocol), a fixed restoration for the patients can be made possible.
The further treatment (2nd corrective operation after 2-4 months) usually includes the removal of some of the implants placed during the 1st corrective operation (which are usually loosened at this point anyway due to overloading) and the new treatment of the then healed bone areas as well as the actual creation of a new one BIPS.
Prior to this treatment option, patients must be informed that the (temporary) integration of removable dentures is also possible as an alternative to this procedure.
If tuberopterygoid screws are loose, they should be removed a few days before the corrective surgery to allow the bone and endosseous (peri-implant) soft tissue to cope with the bacterial load.
Alternative procedure: the new tuberopterygoid screw(s) must not be inserted into the extraction alveoli of the previous tuberopterygoid screws but in nearby bone areas (usually parallel), hence anchoring in the same target cortical.
If it is not possible to anchor new implants in the pterygoid process, several Corticobasal® implants with a larger diameter can alternatively be used in the distal upper jaw.
Since the implants are almost always positioned in a row in segment constructions (and cross-arch stabilization is not possible), the therapeutic options for treating mobility are very limited, especially when considering potential infections in the bone segment. All implants of the segment construction are typically replaced. The most distal implants in the maxilla and mandible have the greatest probability of surviving under these conditions.
| Revision No. | Document name / number | New version | Previous version | Modification | Date of approval | Release by |
|---|---|---|---|---|---|---|
| Rev 1 | 8_EN_Consensus_indications_procedure_corrective_surgery_04-22 | V002 | V001 | Version 2 revised in several areas, based on version 1 from 20.03.2017 | 25.04.2022 | IF Board, for consultation |